



Understanding Breast Augmentation
Breast augmentation is a surgical procedure that uses implants, fat transfer, or a combination of both to alter breast size and shape. It’s one of the most commonly performed cosmetic procedures in Australia, but the term covers a wide range of clinical situations, from a young woman who feels her breasts never developed to her satisfaction, through to a patient in her forties looking to address volume changes after pregnancy or weight loss.
What it cannot do is correct significant sagging on its own. If your nipple sits below the breast crease, an implant alone will sit high on the chest while your tissue continues to hang below it, sometimes producing what surgeons call a double bubble or Snoopy nose deformity. In those cases, a breast lift with implants may be more appropriate. Dr Turner will assess this at your consultation and tell you honestly which approach is likely to suit you.
Understanding Your Anatomy
A lot of patient confusion about implant size comes down to a misunderstanding of the underlying architecture. Breast tissue sits on top of the pectoralis major muscle, which sits on top of the rib cage. The implant is placed somewhere within that layered structure. How it looks afterwards depends as much on what’s underneath as on what implant goes in.
Chest Wall Dimensions
The width and curvature of your rib cage place hard limits on what implant can fit. Two patients with identical breast volume can have very different chest wall shapes, and the same implant in those two patients will look quite different. In clinic, I take detailed measurements of chest width, breast width, and the distance from the breast crease to the nipple before any implant size is even discussed.
Breast Footprint
Your existing breast has a footprint, the area where it sits against the chest wall. Implants that match this footprint tend to give a more proportionate result. Implants that exceed the footprint, particularly in width, can produce visible edges, side fullness that looks unbalanced, and increased pressure on tissues over time.
Tissue Quality and Coverage
Soft tissue thickness over the upper pole determines how much of the implant edge will be visible or palpable. Thin tissue means a higher chance of visible rippling, particularly with smooth round implants placed above the muscle. Thicker tissue gives more options. I assess this with a pinch test at consultation.
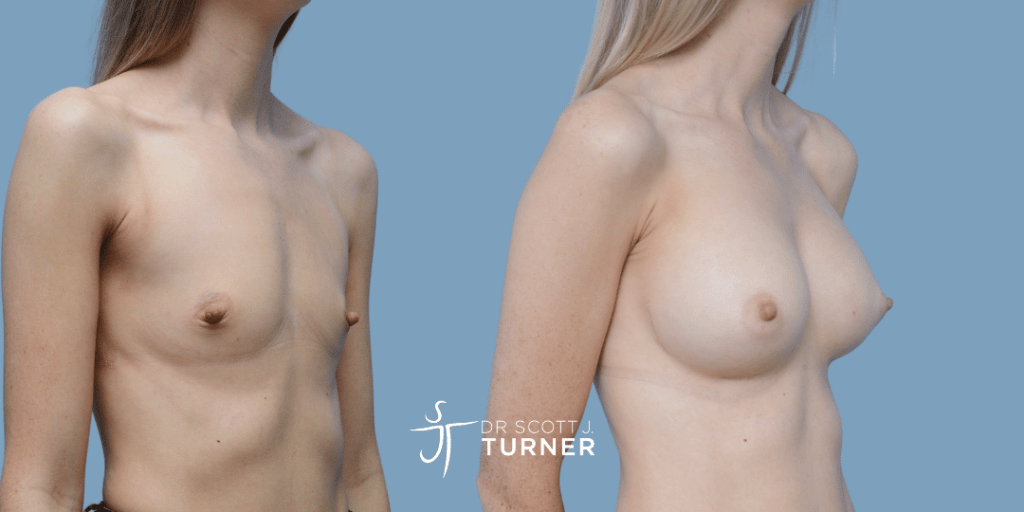
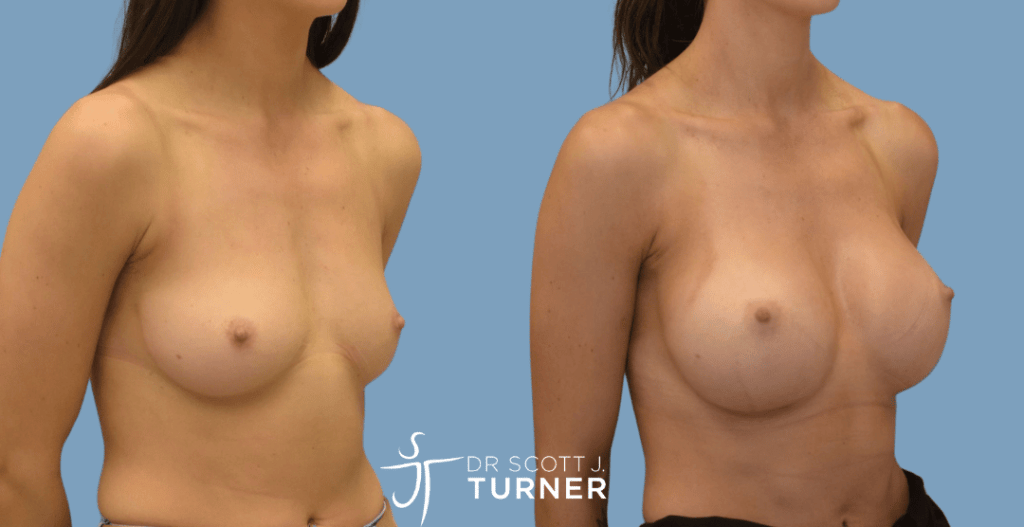
Breast Augmentation Before and After Photos
View breast augmentation before and after photos from Dr Turner’s Sydney patients, including examples of round implants, anatomical implants and results in patients with different body frames and breast shapes. Photos are intended as general examples only. Your own result will depend on your anatomy, implant selection, tissue quality and surgical plan.
View breast augmentation before and after photos
Round Breast Implants
See examples of round breast implants, commonly used for breast augmentation.
View round breast implant before and after photos
Teardrop Breast Implants
View examples of anatomical implant results in selected patients.
View teardrop breast implant before and after photos
Asian Breast Augmentation
See examples of breast augmentation in Asian patients with different tissue and frame considerations.
View Asian breast augmentation before and after photos
Before and after photos are examples only. Results vary between patients and depend on anatomy, tissue quality, implant choice, surgical plan and healing.
Dr Turner’s Approach: Tissue-Based Planning
Tissue-based planning means starting with what your anatomy can support, then working out which implant fits within those parameters. The alternative, which is unfortunately still common in some practices, is to start with a desired cup size and force-fit an implant to achieve it.
The problem with the cup-size-first approach is that cup sizing is not standardised across bra manufacturers, and it tells the surgeon nothing about whether a given implant will actually fit your chest wall safely. Patients who request an implant width significantly beyond their breast footprint often experience higher rates of bottoming out, lateral implant displacement, and tissue thinning over time.
What I aim for is the largest implant that fits comfortably within your existing footprint and tissue coverage, with a profile that suits your chest depth. That’s typically the result that ages best.
How Do I Choose the Right Breast Implants?
There are five variables to work through with every implant decision: brand, size, shape, profile, and surface texture. None of them are independent of each other, which is why the implant conversation typically takes up a substantial portion of the consultation.
Implant Brands: Mentor and Motiva
Dr Turner uses Mentor and Motiva implants exclusively. Both are TGA-approved, both have established long-term safety records, and both are tracked through the Australian Breast Device Registry (ABDR).
Mentor implants are manufactured in the United States and have over 35 years of clinical data behind them. They use a cohesive silicone gel and offer both smooth and Siltex (lightly textured) surfaces. Mentor’s clinical history is extensive and the implants are well-studied.
Motiva implants are a newer Latin American brand that has gained traction internationally over the last decade. They use a softer silicone gel, a SmoothSilk surface, and incorporate technologies like the Q Inside microchip for traceability. Motiva implants typically feel softer to the touch but require careful handling during placement.
Neither brand is universally better. The right choice depends on your tissue characteristics, your preferences around feel and longevity, and the specifics of your case.
Implant Size
Implant size is measured in cubic centimetres (cc), not cup sizes. A 300cc implant in one patient may produce a different visual outcome than the same implant in another patient because of differences in chest wall, tissue coverage, and existing breast volume.
In clinic, we use a Volume Sizing System, sterile sizers placed inside a sports bra, to give you a much more accurate sense of what a given volume will look like on your frame. This is more useful than trying implants in a fitting bra, which doesn’t account for skin expansion or chest wall curvature.
Implant Shape: Round vs Anatomical (Teardrop)
Round implants are symmetrical, they look the same from any angle, and they cannot rotate out of position. Anatomical or teardrop implants have a profile shaped to mimic the natural breast slope, fuller in the lower pole than the upper.
Round implants have become the default for most augmentation patients because cohesive gel technology means modern round implants no longer “balloon” at the top in a way they once did. They also tolerate small amounts of rotation without affecting the result. Anatomical implants can give a particular shape in the right candidate, but they need to stay oriented correctly to look right, and rotation can cause asymmetry that requires revision.
In tuberous breast correction, anatomical implants often play a specific role because of the breast shape they’re correcting. For routine primary augmentation, round is more commonly used in current practice.

Implant Profile and Projection
Profile refers to how far the implant projects forward from the chest wall for a given base width. Implants come in low, moderate, moderate plus, high, and extra high profile options.
Higher profile means more forward projection in a narrower base, which suits women with narrower chest walls who still want forward fullness. Lower profile spreads the same volume over a wider base, which suits broader chests or patients wanting a more spread look. Profile selection is one of the more nuanced parts of implant choice and is best worked out during consultation rather than predetermined.
Implant Surface: Smooth vs Textured
Smooth implants have a polished outer shell. Textured implants have a roughened surface designed to grip surrounding tissue and reduce rotation in anatomical implants. Aggressive macrotextured implants (Allergan Biocell, recalled in 2019) were associated with the majority of BIA-ALCL cases globally.
Modern textured options like Siltex are classified as microtextured and have a substantially lower BIA-ALCL signal than the recalled macrotextured options. Smooth implants have not been associated with BIA-ALCL. For most patients, Dr Turner uses smooth implants. Textured options are considered when there’s a specific clinical reason, such as preventing rotation in an anatomical implant.

Implant Comparison Table
| Feature | Round | Anatomical (Teardrop) |
|---|---|---|
| Shape | Symmetrical | Asymmetrical (lower pole fuller) |
| Rotation tolerance | Will tolerate rotation | Must stay oriented |
| Upper pole fullness | More | Less |
| Cleavage | Stronger projection | More natural slope |
| Most common surface | Smooth | Textured (to prevent rotation) |
| Typical use | Primary augmentation | Tuberous correction, specific aesthetic |
Am I a Suitable Candidate?
Suitability for breast augmentation is more than wanting larger or differently shaped breasts. It depends on your anatomy, your physical health, your psychological readiness, and your understanding of what surgery can and cannot achieve.
Anatomical Considerations
You may be a candidate if:
- Your breast development is complete (typically age 18 or older for cosmetic indications)
- You have adequate soft tissue coverage to support an implant
- Your nipple position sits at or above the breast crease, or your asymmetry is mild
- You have no significant ptosis (sagging) requiring a lift
- Your chest wall does not have severe asymmetry or deformity that would require reconstructive rather than cosmetic surgery
If you have significant ptosis, you may need a breast lift with implants rather than augmentation alone. Dr Turner will assess this with a physical examination at consultation.
Lifestyle and Health Factors
You’ll need to be:
- In good general health, with conditions like diabetes well-controlled
- At a stable weight, ideally near your long-term target weight
- A non-smoker, with smoking and vaping ceased for at least six weeks before and after surgery (smoking dramatically increases complication rates)
- Free of active infection or wound healing conditions
- Realistic about what surgery can achieve and what it cannot
If you’re planning future pregnancies, this is worth discussing in consultation. Pregnancy and breastfeeding can change breast volume and tissue elasticity in ways that affect long-term results. There’s no medical reason to wait, but some women prefer to defer surgery until their family is complete.
The Two-Consultation Process and Cooling-Off Period
Since the AHPRA cosmetic surgery reforms came into effect in July 2023, every patient considering cosmetic breast augmentation must:
- Obtain a GP referral before the first consultation. Your GP provides a letter confirming your medical history, current medications, and any conditions that may affect surgery.
- Attend a minimum of two consultations with Dr Turner before surgery is booked. Dr Turner conducts these consultations personally. There are no patient representatives or coordinators standing in.
- Undergo a psychological assessment to confirm readiness for surgery and screen for conditions like body dysmorphic disorder.
- Wait at least seven days between your final consultation and your surgery date. This is the cooling-off period mandated by AHPRA, and it’s there to ensure no patient feels pressured into a same-week decision.
Some patients find these requirements frustrating, particularly if they’ve been considering surgery for years. The intent is patient safety, and in practice the structured process tends to produce well-considered decisions and better long-term satisfaction.
How Is Breast Augmentation Surgery Performed?
Breast augmentation is performed under general anaesthetic in a fully accredited private hospital, with a specialist anaesthetist providing care throughout. The procedure typically takes between 60 and 90 minutes for a standard primary augmentation, longer if a lift is added or if revision work is involved.
Most patients are discharged the same day. Some prefer an overnight stay and that’s available, particularly for patients travelling from interstate or those who would prefer monitored first-night recovery.
Incision Options
There are three incision options used internationally for breast augmentation. Each has trade-offs.
Inframammary Fold Incision
The inframammary fold (IMF) incision sits in the natural crease beneath the breast. This is Dr Turner’s preferred approach for most primary augmentations. The scar is hidden in the crease and typically fades to a fine line within 12 to 18 months.
Advantages: precise pocket dissection, direct access for implant placement, the lowest rate of capsular contracture compared with other incisions, and the ability to use any implant size or shape.
Trade-off: there is a visible scar in the breast crease. For most women, the trade-off is acceptable because the scar is genuinely hidden in normal posture and clothing.
Periareolar Incision
The periareolar incision sits at the lower border of the areola, where pigmented skin meets breast skin. The scar can blend well into the colour transition, but the incision passes through breast tissue and milk ducts, which slightly increases capsular contracture rates and may affect breastfeeding ability.
This option is sometimes considered for patients who are also having a periareolar lift component, where the scar is being placed there anyway.
Trans-Axillary Incision (Why Dr Turner Does Not Use This Approach)
The trans-axillary incision is placed in the armpit. The advantage promoted is that there’s no scar on the breast itself.
In practice, the disadvantages are significant enough that Dr Turner does not use this approach. Pocket dissection is more difficult through a remote incision, which can affect implant positioning. Bleeding control is harder. The approach historically was used for saline implants placed empty and filled in situ, which is not how modern silicone gel implants work. And the armpit scar is often visible in singlet tops and swimwear, particularly in patients who tan.
If you’ve read about trans-axillary augmentation elsewhere, this is the reason you won’t be offered it as an option in our practice.
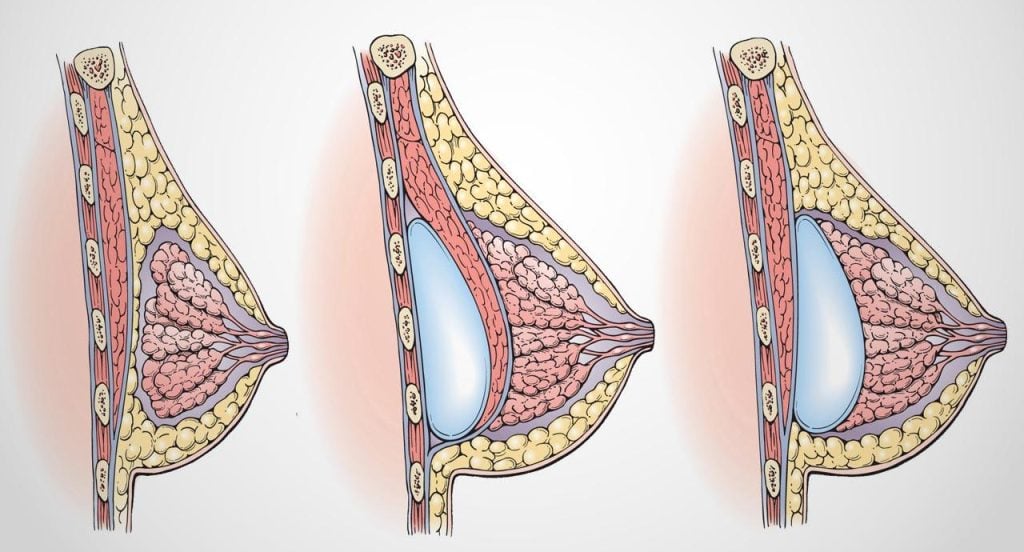
Implant Placement Options
Where the implant sits relative to the pectoralis major muscle is a separate decision from where the incision is placed. There are three options.
Subglandular (Above the Muscle)
The implant sits directly behind the breast tissue, above the pectoralis major. This may suit patients with adequate soft tissue coverage in the upper pole and faster recovery.
Trade-offs: higher visibility of implant edges in thin patients, slightly higher capsular contracture rates, and greater interference with mammographic imaging. Less commonly used in current practice for primary augmentation.
Submuscular (Under the Muscle)
The implant sits behind the pectoralis major muscle. This provides additional soft tissue coverage in the upper pole and reduces the visibility of implant edges. Capsular contracture rates are lower with this approach.
Trade-offs: longer initial recovery because the muscle has been lifted, and animation deformity (visible movement of the implant when the pectoral muscle contracts) can occur in some patients.
Dual Plane (Most Commonly Used)
Dual plane is a refinement of submuscular placement where the upper portion of the implant sits beneath the muscle and the lower portion sits behind breast tissue alone. This combines the upper pole coverage of submuscular placement with the more natural lower pole behaviour of subglandular placement.
For most primary augmentation patients, dual plane is the placement Dr Turner recommends.
The Internal Bra Technique
The Internal Bra is a refinement of standard breast augmentation that uses absorbable mesh or biological scaffold to provide additional internal support to the lower pole and lateral aspects of the breast. Think of it as a sling that supports the implant from inside, taking some of the long-term load off the skin envelope and the inframammary fold.
In practice, this technique may help reduce the rate of bottoming out (where the implant gradually descends below the natural breast crease over time), help maintain projection in patients with thin or stretched skin, and provide additional structural support in revision cases where previous tissue has thinned.
The technique adds a small amount to operative time and to surgical complexity. It’s not necessary for every primary augmentation. For patients with thin skin, weak inframammary fold support, or anatomy that would be difficult to support long-term with skin alone, the internal bra can make a meaningful difference to durability of the result.
Dr Turner discusses internal bra suitability case by case at the planning stage.
Hybrid Breast Augmentation
Hybrid breast augmentation combines an implant with fat transfer in the same procedure. The implant provides the underlying volume and projection. The transferred fat (harvested from another body area through liposuction) fills the upper pole, softens the implant edges, and addresses any small contour irregularities or asymmetries.
The hybrid approach may suit patients with very thin tissue coverage, patients with mild upper pole hollowness, and those wanting a softer transition from chest wall to breast. It does add operative time and recovery in two body areas.
Not every patient is a hybrid candidate. The fat donor area needs to have enough fat for harvest, and the patient needs to be a stable weight (significant weight loss after the procedure can reduce the volume of transferred fat).
Dr Turner’s 12-Point Surgical Protocol
What happens in the operating theatre matters as much as what was planned in the consultation room. The following protocol is followed for every primary breast augmentation Dr Turner performs.
- Pre-operative antibiotic prophylaxis administered intravenously by the anaesthetist
- Antiseptic skin preparation with chlorhexidine, with full draping of the operative field
- Precise marking of incision lines, breast crease, and asymmetry adjustments while the patient is awake and standing, before anaesthesia
- Inframammary fold incision at the planned location, with careful dermal closure planning
- Pocket dissection under direct vision with diathermy haemostasis, no blunt dissection beyond what’s needed for implant placement
- Triple antibiotic pocket irrigation with cefazolin, gentamicin, and povidone-iodine solution as per the 14-point plan published internationally for capsular contracture prevention
- Glove change and re-prep before implant handling to reduce bacterial contamination of the implant surface
- Keller Funnel insertion of the implant, a sterile cone-shaped device that allows no-touch placement and reduces surface contamination during insertion
- Implant orientation check with the patient briefly tilted upright to assess symmetry before final closure
- Layered closure with absorbable sutures in deep dermis and subcuticular layers, no external sutures requiring removal
- Surgical bra application in theatre before the patient wakes
- Documentation in the Australian Breast Device Registry (ABDR) for long-term tracking, with implant batch numbers recorded
Some surgeons follow a similar protocol. Others vary in their approach. What you should look for is consistency: a surgeon who can articulate exactly what they do at each stage and why.
Recovery and Aftercare
Recovery is the part of the journey patients tend to underestimate. The surgery itself takes about 90 minutes. The recovery is a phased process that runs across several months.
First Week
The first 48 to 72 hours are the most uncomfortable. You’ll experience tightness across the chest, particularly with submuscular or dual plane placement. Pain is typically managed with prescription medication for the first 4 to 5 days, then over-the-counter analgesia.
You’ll need someone at home with you for at least the first 24 hours. No driving for at least a week, longer if you’re still taking opioid pain medication. Sleeping on your back with your head elevated on two or three pillows is recommended for the first two weeks.
A surgical bra is worn 24/7 from theatre, removed only briefly for showering after day 3.
Weeks 2 to 6
Most patients return to office-based work after 7 to 10 days. Heavier lifting (over 5kg), upper body exercise, and any activity that engages the pectoral muscle is restricted for six weeks.
Swelling subsides progressively over this period, but final settling takes longer. The implant typically sits high on the chest in the first 2 to 3 weeks before beginning to drop into its final position. This is normal and expected.
Drop and Fluff: How Implants Settle
Drop and fluff describes the process by which implants gradually move from their initial high position into their final settled position over the first 3 to 6 months. The “drop” refers to vertical settling as the lower pole skin and pectoral muscle relax. The “fluff” refers to the softening of the implant pocket and the transition from a tight, high look to a softer, more rounded final shape.
If your breasts look high and tight at week 2, this is expected. Patience is the right response, not concern. Most settling is complete by 3 months, with final shape settling at around 6 months.
Scar Management
Scars on the breast typically take 12 to 18 months to mature. During that time:
- Silicone scar therapy (gel or sheet) starting at 3 weeks post-op
- Sun protection over the scar for 12 months (UV exposure causes hyperpigmentation)
- Massage techniques as instructed at follow-up
- Laser scar treatment may be available if scars become hypertrophic
Return to Work and Exercise
| Activity | Typical timing |
|---|---|
| Office-based work | 7 to 10 days |
| Light walking | From day 1 (encouraged) |
| Driving | 1 to 2 weeks (off pain medication) |
| Lower body exercise (legs only) | 3 to 4 weeks |
| Upper body exercise / chest work | 6 to 8 weeks |
| High-impact running / jumping | 6 to 8 weeks (with appropriate sports bra) |
| Sleeping on side | 3 weeks |
| Sleeping on stomach | 6 weeks |
Follow-up appointments are scheduled at 1 week, 1 month, 3 months, 6 months, and 1 year, all in person at the Sydney clinic.
Risks and Complications
Every surgical procedure carries risks. Breast augmentation is generally considered safe, but the risks are real and need to be understood before any decision is made.
General Surgical Risks
These apply to any surgery performed under general anaesthetic:
- Adverse reaction to anaesthetic agents
- Infection at the incision site
- Bleeding or haematoma formation
- Wound healing problems
- Deep vein thrombosis (rare with appropriate prevention)
Procedure-Specific Risks
- Capsular contracture: scar tissue around the implant tightens, causing firmness, distortion, and sometimes pain. Current rates with modern technique sit around 5% over 10 years.
- Implant malposition: the implant settles in the wrong position. May require revision surgery.
- Bottoming out: the implant gradually descends below the breast crease over time.
- Rippling: visible or palpable folds in the implant, more common in thin patients with smooth round implants placed above the muscle.
- Changes in nipple sensation: approximately 10 to 15% of patients experience some change. Most resolves over 12 months. Permanent change occurs in around 10% of cases.
- Implant rupture: silicone implants can rupture from trauma or over time. Modern cohesive gel means leakage is contained within the capsule rather than dispersing.
- Asymmetry: some natural asymmetry typically remains. Significant asymmetry is uncommon but can occur.
- Need for revision surgery: approximately 20% of breast augmentation patients will undergo revision surgery within 10 years for various reasons.
How Dr Turner Reduces Risk
Risk reduction is built into the 12-point surgical protocol. Specifically:
- Triple antibiotic pocket irrigation reduces capsular contracture rates
- Keller Funnel placement reduces bacterial contamination of the implant surface
- Smooth implants are used preferentially based on long-term safety data
- Patients are screened for risk factors before surgery (smoking cessation, weight stability, condition control)
- ABDR registration provides traceability if any future safety signal emerges with a specific implant model
No surgeon can eliminate risk. What we can do is apply each evidence-based step that reduces it.
Breast Augmentation Cost in Sydney
Breast augmentation cost in Sydney depends on the type of procedure performed and whether additional techniques are needed to achieve a stable, natural-looking result. A straightforward implant-only breast augmentation is usually less complex than a hybrid breast augmentation with fat transfer, correction of asymmetry, tuberous breast features, or breast augmentation combined with a lift.
As a general guide:
-
Standard breast augmentation with implants: from $11,000 all-inclusive. This covers straightforward implant-only breast augmentation using premium implants such as Motiva, Mentor or equivalent, general anaesthetic, private hospital theatre time and routine follow-up care. It is most suitable for patients with good skin quality, adequate breast tissue and no significant sagging who want to add breast volume with implants alone.
-
Hybrid breast augmentation with implants and fat grafting: from $15,000 all-inclusive. This combines breast implants with fat transfer, usually harvested from areas such as the abdomen, flanks or thighs. Fat grafting may help improve soft tissue coverage over the implant, refine the upper pole transition and soften contour irregularities. The higher cost reflects the additional operating time and the fact that surgery is performed in both the breast and donor areas.
Factors that may affect the total cost include implant choice, whether fat grafting is added, whether internal bra support is recommended, the degree of asymmetry or tuberous breast correction required, and the total operating time needed for your anatomy and surgical plan.
Breast augmentation is usually a cosmetic procedure and is not eligible for Medicare rebates or private health insurance benefits. Limited rebates may apply only in specific reconstructive or recognised developmental conditions, such as reconstruction after mastectomy or selected congenital breast conditions that meet Medicare criteria.
You will receive a personalised written quote after consultation with Dr Turner. This quote outlines the expected surgeon, anaesthetist, hospital, implant and follow-up costs based on your individual procedure plan.
For a broader breakdown of pricing across breast procedures, see the guide to breast surgery costs in Sydney.
Frequently Asked Questions
How long does breast augmentation surgery take?
Primary breast augmentation typically takes between 60 and 90 minutes in the operating theatre. Procedures involving fat transfer, hybrid augmentation, or breast lift components take longer. The full theatre time, including anaesthesia and emergence, is usually around 2 hours.
Will I be able to breastfeed after breast augmentation?
Most patients retain the ability to breastfeed after breast augmentation. The inframammary fold incision avoids breast tissue and milk ducts, which is one reason it’s preferred over the periareolar approach in patients planning future pregnancies. That said, no surgical approach can guarantee preservation of breastfeeding capacity, and some patients do experience reduced supply after augmentation.
How long do breast implants last?
Modern silicone implants do not have a fixed expiry date. The historical 10-year replacement myth has been replaced with monitoring-based recommendations: regular review with your surgeon, MRI or ultrasound surveillance from 5 to 6 years onwards as recommended by the FDA, and replacement only when clinically indicated. Many patients keep the same implants for 15 to 20 years or longer. See the implant lifespan article for detail.
When can I return to work after breast augmentation?
Most patients with office-based work return at 7 to 10 days. Patients with physically demanding jobs that involve lifting, reaching overhead, or chest engagement need 4 to 6 weeks before returning to full duties. Plan for at least two weeks off work for any role that involves more than seated computer work.
When can I exercise after breast augmentation?
Light walking is encouraged from day 1. Lower body strength training can resume at 3 to 4 weeks. Upper body and chest work waits until 6 to 8 weeks. High-impact running and jumping resumes at 6 to 8 weeks, with appropriate sports bra support. The full return-to-exercise timeline is covered in the exercise after breast augmentation article.
Will breast augmentation affect mammograms?
Breast implants do affect mammographic imaging. Standard mammograms still work, but additional displacement views (Eklund views) are needed to image breast tissue around the implant. Letting your imaging provider know you have implants is essential. For high-risk screening, MRI may be more useful than mammogram alone.
What is the recovery time for breast augmentation?
Active recovery (return to work, normal daily activities) is approximately 2 weeks. Full recovery, including return to all exercise and full implant settling, is 8 to 12 weeks. Final settling and shape stabilisation continues out to 6 months. See the recovery after breast augmentation article for detail.
Is breast augmentation covered by Medicare?
Cosmetic breast augmentation is not covered by Medicare. There are limited circumstances where Medicare item numbers may apply, primarily reconstruction following mastectomy or for specific congenital conditions like tuberous breast deformity in some cases. Standard cosmetic augmentation is paid privately. See breast surgery costs for fee structure detail.
Consult with Dr Scott J Turner in Sydney
Dr Scott J Turner is a Specialist Plastic Surgeon (FRACS) consulting at his Bondi Junction and Manly clinics in Sydney. Surgery is performed at accredited private hospitals in Sydney, including Bondi Junction Private Hospital, Delmar Private Hospital in Dee Why, and East Sydney Private Hospital.
Dr Turner has more than a decade in private practice focused on cosmetic surgery and has performed more than 1,000 breast procedures. His approach to breast augmentation is based on tissue-based planning, careful assessment of breast width, chest wall shape, tissue quality and implant support, rather than selecting implants by cup size alone.
Every consultation is conducted personally by Dr Turner. There are no patient representatives or coordinators standing in for the surgeon. A minimum of two consultations is required before any surgery is booked, in line with AHPRA requirements. Cosmetic surgery patients also require a GP referral, psychological screening and a mandatory cooling-off period before proceeding.
Breast augmentation is planned using TGA-approved implants, such as Mentor and Motiva, with implant selection based on your anatomy, preferences and surgical goals. Dr Turner uses a structured surgical protocol that includes accredited hospital care, specialist anaesthetic support, careful implant handling and registration with the Australian Breast Device Registry for long-term traceability.
Consultations are unhurried, focused on careful clinical assessment, and structured around honest discussion of what surgery can and cannot achieve in your specific situation.
If you’re considering breast augmentation, the next step is to obtain a GP referral and book an initial consultation. Contact the practice on [email protected] or via the contact page to begin the process.







